Carpal Tunnel Syndrome
Carpal Tunnel Syndrome, Shoulder & Leg Pain
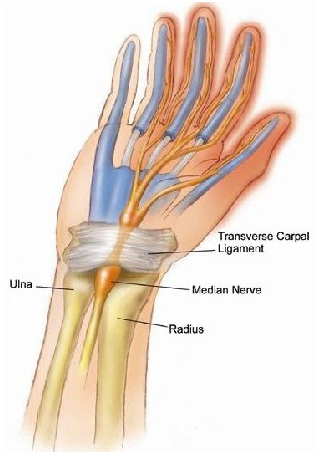
The traditional medial concept of carpal tunnel syndrome is that the symptoms of hand numbness, pain, swelling and tingling is due to a compression of the median nerve at the carpal tunnel by the transverse carpal ligament. The carpal tunnel is a small tunnel made of wrist bones through which the median nerve passes. The transverse carpal ligament crosses over the top of the tunnel to help support its structure. There are several reasons why compression at the carpal tunnel can occur including collapse of the tunnel itself, subluxation of the carpal bones of the tunnel, proliferation of the cartilage in the tunnel, connective tissue adhesions on the nerve in the tunnel, inflammation in the tunnel, and inflammation and swelling of the nerve in the tunnel. This has been treated traditionally by cutting the transverse carpal ligament surgically to free the entrapment.
There are several problems with this approach. First, common sense will tell you that cutting the transverse ligament will leave the structure of the wrist in a weakened condition. Secondly, this approach does not really address the reason for the compression in the first place, only relieving the symptoms by taking pressure off the nerve. Thirdly, most of these problems can be resolve easily with conservative care, making surgical intervention an outdated and unnecessary procedure. Also, keep in mind, that surgery does not always work (11)(12)(13)(14)(24). In addition, conservative care, which I will describe, is far cheaper than surgery. The usual routine of sending the patient for 6 weeks of physical therapy followed by wrist surgery is a tremendous waste of money.
I am going to make a bold statement – In most cases carpal tunnel is an understood and resolvable problem with chiropractic care. While there is an ongoing debate in the research literature about which surgery is best (2)(13), when surgery should be performed (3), weather surgery is better than conservative care (4)(16)(5)(25), or what the exact nature of the injury is, I believe the easy solution to this problem can be demonstrated to any reasonable person in a very short time. In our office we can greatly improve or resolve most of these problems in 1 to 5 visits.
There are some that take much more, but there are usually reasons for it. The more damaged and inflamed the tissues, the longer it takes to heal. If the muscles in the arm have become hardened and fibrotic, it will take time to rehabilitate them. But heal it will once the conditions are set for it to happen. It has been proposed that the best candidates for surgery are young patients with symptoms presenting for less than 1 year (3). In our opinion these individuals are not candidates for surgery at all and are the easiest to fix with chiropractic technology.
To describe why traditional medical solutions to this problem are inappropriate, let me start by saying that the entire field of healing is undergoing a transition from the “old medicine” to the “new medicine”. Old medicine is the practice of describing a body disturbance with a ‘diagnosis’ and coming up with a solution to the diagnosis in the form of a prescription, weather it be a drug, physical therapy or whatever. New medicine is the practice of uncovering malfunctions in various systems of the body which produce the imbalances and breakdowns we call disease. There are usually many factors involved, not one. These are treated by correcting the malfunctions. There is no absolute line between these 2 approaches, but the general strategic differences between them are like night and day. This new approach is called Functional Medicine.
The traditional approach to Carpal Tunnel is to regard it as primarily a wrist problem and many orthopedists still treat it as such. There have been various studies which have offered convincing ideas and data that contradict this. In 1973 Upton & McComas (3)(18)(26)(27) presented the theory that of the ‘double crush syndrome’, the idea that a nerve could be interfered with at more than one location along its course, with each interference  causing a sub-clinical disturbance. The effects of each disturbance are additive. This means that each interference, by itself, would not cause a problem, but both together would. These interference block what is called axoplasmic flow, the migration of substances down the length of the nerve. Nerves feed tissues, they
causing a sub-clinical disturbance. The effects of each disturbance are additive. This means that each interference, by itself, would not cause a problem, but both together would. These interference block what is called axoplasmic flow, the migration of substances down the length of the nerve. Nerves feed tissues, they
don’t just stimulate muscle contraction. Without proper nerve innervation, joints and other tissues will degenerate. While this idea is still debated in the literature, there is considerable evidence supporting it (3)(6)(9)(18)(20). I am personally sold on this idea. This ‘double crush’ idea lays the foundation for understanding the non-local causes of carpal tunnel.
But there is more to the story. Other researchers have noted that carpal tunnel symptoms are part of a general syndrome of the upper extremities (1)(9) (12)(17)(19)(21)(22)(24)(26). Systemic metabolic problems such as diabetes (27) or postural misalignments of the shoulders and head (19) have also been determined to be factors. It takes little imagination to realize that this list will be extended as research continues. To get straight to the bottom line, carpal tunnel is one of the symptoms of general neck/shoulder/arm dysfunction, and often including systemic factors such as inflammation, and should be addressed by correcting the entire malfunction. In our experience it is not unusual to address perhaps 20 or more disturbances to allow the upper extremity to function properly and carpal tunnel to resolve. Many can be corrected in a few seconds. Some take more time. But an amazing amount can be done in 20 to 30 minutes of treatment. It is also worth noting that the same techniques that work on carpal tunnel also work on other related problems such as tendonitis, shoulder pain, tennis elbow and myofascial pain in the upper extremities. In fact, it is not uncommon to have to resolve these issues as part of the carpal tunnel solution.
Although not fully appreciated by most insurance companies, or the medical field, much of the effective technology for addressing this problem as been developed within the Chiropractic field. Building on the earlier work of Ida Rolf PhD, sophisticated understanding and techniques for correcting the myofascial aspects of this problem have been developed by Michael Leahy DC, and presented as Active Release Technique (ART). In a recent seminar he stated that he had been able to reduce medical costs in 30 corporations by 80% using ART. Diagnostic, neuro-muscular and nutritional considerations have been highly evolved by George Goodheart DC and his associates within the field of Applied Kenisiology. Traditional chiropractic manipulation of the spine and extremities can play a significant roll where appropriate (5) (7)(16). There is also a roll for physical therapy, stress reduction, exercise and proper training in use of the body (4)(16). In most cases, carpal tunnel involves only short term care.
Footnotes:
1. Atroshi, I., Gummesson, C., Johnsson, R., Ornstein, E., Ranstam, J., Rosen, I., “Prevalence of carpal tunnel syndrome in a general population,” JAMA. 1999 Jul 14;282(2):153-8.
Comment: Symptoms of pain, numbness and tingling are common in the general population, and about 1 in 5 are due to carpal tunnel.
2. Burke, DT., Burke, M.A., Bell, R., Stewart, G.W., Mehdi, R.S., Kim, H.J.,”Subjective swelling: a new sign for carpal tunnel syndrome.” Am J Phys Med Rehabil. 1999 Nov-Dec;7,8(6):504-8.
Comment: Swelling in the affected hand is an important diagnostic symptom for the assessment of carpal tunnel.
3. Baba, H., Maezawa, Y., Uchida, K., Furusawa, N., Wada, M., Imura, S., Kawahara, N., Tomita, K., “Cervical myeloradiculopathy with entrapment neuropathy: a study based on the double crush concept.” Spinal Cord. 1998 Jun;3,6(6):399-404.
Comment: Findings for surgical release of cervical compression as well as peripheral ones.
4. Crawford, J.Ol, Laiou, E., “Conservative treatment of work-related upper limb disorders – a review.” : Occup Med (Lond). 2006 Aug 11; [Epub ahead of print]
Comment: “There was no evidence found to support or refute conservative treatment of tenosynovitis, tendonitis, de Quervan’s disease or diffuse non-specific ULDs.”
5. Davis, P.T., Hulbert, J.R., Kassak, K.M., Meyer, J.J., “Comparative efficacy of conservative medical and chiropractic treatments for carpal tunnel syndrome: a randomized clinical trial.” J Manipulative Physiol Ther. 1998 Jun;21(5):317-26.
Comment: “Carpal tunnel syndrome associated with median nerve demyelination but not axional degeneration may be treated with commonly used components of conservative medical or chiropractic care.”
6. Dellon, A.L., Mackinnon, S.E., “Chronic nerve compression model for the double crush hypothesis.” Ann Plast Surg. 1991 Mar;26(3):259-64.
Comment: “This study confirms that the existence of two sites of simultaneous compression, or a second (later) site of compression, placed either proximal or distal to the first (earlier) site of compression, will result in significantly poorer neural function than will a single site of compression.”
7. Flatt, D.W., “Resolution of a double crush syndrome.” J Manipulative Physiol Ther. 1994 Jul-Aug;17(6):395-7.
Comment: Case history of a successful chiropractic treatment of low back pain and leg numbness using the double crush hypothesis.
8. Garfinkel, M.S., Singhal, A., Katz, W.A., Allan, D.A., Reshetar, R., Schumacher H.R., Jr., “Yoga-based intervention for carpal tunnel syndrome: a random trial.” JAMA. 1998 Nov 11;280(18):1601-3.
Comment: Yoga-based therapy was more effective than wrist splinting or no treatment in relieving some symptoms of carpal tunnel.”
9. Gozke, E., Dortcan, N., Kocer, A., Cetinkaya, M., “Ulnar nerve entrapment at wrist associated with carpal tunnel syndrome.” Neurophysiol Clin. 2003 Nov;33(5):219-22.
Comment: 18% of those with carpal tunnel also had signs of ulnar nerve entrapment.
10. Gupta, S.K., Benstead, T.J., “Symptoms experienced by patients with carpal tunnel syndrome.” Can J Neurol Sci. 1997 Nov;24(4):338-42.
Comment: Sensory symptoms outside the distribution of the medial nerve are common in CTS.
11. Hobby, J.L., Venkatesh, R., Motkur, P., “The effect of age and gender upon symptoms and surgical outcomes in carpal tunnel syndrome.” J Hand Surg [Br]. 2005 Dec;30(6):599-604. Epub 2005 Sep.
Comment: “The majority of patients over the age of 70 reported an improvement in symptoms and function, but they were less satisfied with their treatment than younger patients. Some patients had problems with persistent numbness and loss of dexterity following surgery.”
12. Lee, MJ, LaStayo, PC, “Pronator syndrome and other nerve compressions that mimic carpal tunnel syndrome”, J Orthop Sports Phys Ther. 2004 Oct;34(10):601-9.
Comment: Carpal tunnel symptoms that do not respond to therapy may be due to pronator syndrome.
13. Lorgelly, PK, Dias, JJ, Bradler, MJ, Burke, FD. “Carpal tunnel syndrome, the search for a cost-effective surgical intervention: a randomized controlled trial”. Ann R Coll Surg Engl. 2005 Jan;87(1):36-40.
Comment: To read between the lines, the discussion here that one type of surgery does not remove symptoms any better than another suggests that neither surgery is successful in removing symptoms.
14. Mateicik, V. “Entrapment syndromes of the peripheral nerves of the upper extremities”. Rozhl Chir. 2002 Nov;81(11):567-73.
Comment: Surgery works better on patients under 30 years old and with symptoms lasting less than 1 year.
15. Macdermaid, JC, Wessel, J. “Clinical diagnosis of carpal tunnel syndrome: a systematic review”. J Hand Ther. 2004 Apr-Jun;17(2):309-19.
Comment: various evaluation procedures for carpal tunnel
16. O’Connor, D., Marshall, S., Massy-Westropp N., Non-Surgical Treatment (other than steroid injection) for carpal tunnel syndrome”. : Cochrane Database Syst Rev. 2003;(1):CD003219.
Comment: “Evidence shows significant short-term benefit from oral steroids, splinting, ultrasound, yoga and carpal bone mobilization. Other non-surgical treatments do not produce significant benefit.”
17. Nora, DB., Becker, J., Ehlers, JA., Goomes, I., “What symptoms are truly caused by median nerve compression in carpal tunnel syndrome?” Clin Neurophysiol. 2005 Feb;116(2):275-83.
Comment: “We believe that the variability in the clinical presentation of CTS is largely due to the presence of associated diseases”.
18. Osterman, AL., “The double crush syndrome”. : Orthop Clin North Am. 1988 Jan;19(1):147-55.
Comment: Presents the case that more than one area needs to be treated to resolve carpal tunnel.
19. Pascarelli, EF., Hsu, YP., “Understanding work-related upper extremity disorders: clinical findings in 485 computer users, musicians, and others”. J Occup Rehabil. 2001 Mar;11(1):1-21.
Comment: A total upper body examination is necessary to evaluate carpal tunnel.
20. Raps, SP., Rubin, M., “Proximal median neuropathy and cervical radiculopathy: double crush revisited”. Electromyogr Clin Neurophysiol. 1994 Jun;34(4):195-6.
Comment: Evidence for double crush.
21. Rosenbaum, R., “Disputed radial tunnel syndrome”. Muscle Nerve. 1999 Jul;22(7):960-7.
Comment: Attempts to separate radial tunnel from carpal tunnel.
22. Shimizu, K., Iwasaki, R., Hoshikawa, H., Yamamuro, T., “Entrapment neuropathy of the palmar cutaneous branch of the median nerve by the fascia of flexor digitorum superficialis”. J Hand Surg [Am]. 1988 Jul;13(4):581-3.
Comment: Case reflecting the need to release more than one area to relieve symptoms of carpal tunnel.
23. Valente, R., Gibson, H., “Chiropractic manipulation in carpal tunnel syndrome”. J Manipulative Physiol Ther. 1994 May;17(4):246-9.
Comment: Case history demonstrating positive effects of chiropractic on carpal tunnel.
24. Werner, CO, Rosen, I, Thorngren, KG., “ Clinical and neurophysiological characteristics of the pronator syndrome”. Clin Orthop Relat Res. 1985 Jul-Aug;(197):231-6.
Comment: Failed carpal tunnel surgeries due to lack of consideration to the double crush phenomena.
25. Wilson, JK, Sevier, TL, “A review of treatment for carpal tunnel syndrome”. Disabil Rehabil. 2003 Feb 4;25(3):113-9.
Comment: Long term benefits of conservative medical care have been poor.
26. Wood, VE., Biondi J., “Double-crush nerve compression in thoracic-outlet syndrome”. J Bone Joint Surg Am. 1990 Jan;72(1):85-7.
Comment: More evidence for the double crush hypothesis.
27. Zahir, KS., Zahir, FS., Thomas, JG., Dudrick, SJ., “The double-crush phenomenon-an unusual presentation and literature review”. Conn Med. 1999 Sep;63(9):535-8.
Comment: Metabolic problems contributing to a disturbance of axoplasmic flow and thus double crush.